


Understanding the Health Benefits of Vitamin D
Dr. Sunil J Wimalawansa explains why vitamin D is vital for overall health, playing key roles in musculoskeletal, immune, and cardiovascular functions.

By Sunil J Wimalawansa, MD, PhD, MBA, DSc. Prof. Medicine, Endocrinology & Human Nutrition
Vitamin D is vital for overall health, playing key roles in musculoskeletal, immune, and cardiovascular functions. Its active form, calcitriol, regulates calcium balance and is synthesized in peripheral cells in response to immune signals. Vitamin D, essential for human survival, plays protective and regulatory roles across all body systems. Its most active metabolite, calcitriol [1,25(OH)₂D], functions through two primary mechanisms: intracellular signaling via intracrine and paracrine pathways and genomic actions mediated by its receptors. For these effects to occur, calcitriol must be synthesized within peripheral target cells, as its circulating levels are over 900-fold lower than the concentration required to diffuse into them. In contrast, the hormonal form of calcitriol is synthesized in renal tubular cells and released into circulation. Optimal serum 25(OH)D levels (40-80 ng/mL) are essential for preventing infections, autoimmune diseases, and chronic conditions. However, based on flawed studies and biases, current guidelines fail to address its broader benefits. Optimal 25(OH)D levels discussed here can be achieved via personalized supplementation strategies based on body weight or BMI. Addressing vitamin D deficiency through supplementation and public health initiatives can reduce disease burden, improve health outcomes, and lower healthcare costs.

Hormonal calcitriol primarily regulates calcium homeostasis, parathyroid gland function (via calcium-sensing receptors), and musculoskeletal health. In contrast, non-hormonal calcitriol is synthesized in peripheral target cells, such as immune cells, alongside the production of its receptors (VDR/CTR). Unlike renal tubular cells, which maintain continuous calcitriol production in a steady state, peripheral target cells synthesize calcitriol intermittently in response to chemical signals from cell-surface immune recognition receptors following antigenic or microbial threats. These pattern-recognition receptors, such as Toll-like receptors, are distributed throughout the body. The following sections outline recent discoveries and advancements in understanding the vitamin D/CTR system and its role in human protection.
Calcitriol Systems: Mechanisms and Requirements

Since circulating calcitriol is present in picomolar concentrations—significantly lower than vitamin D₃ and 25(OH)D in nanomolar ranges—its ability to diffuse against a concentration gradient is negligible and clinically insignificant [2, 3]. As a result, calcitriol synthesized in the kidneys or administered pharmacologically (i.e., calcitriol or its 1α-analogs) does not effectively enter peripheral target cells [4]. These cells, therefore, rely on circulating vitamin D₃ and 25(OH)D to meet their functional requirements. Consequently, physicians should avoid prescribing calcitriol or its analogs for conditions other than chronic kidney disease [5].
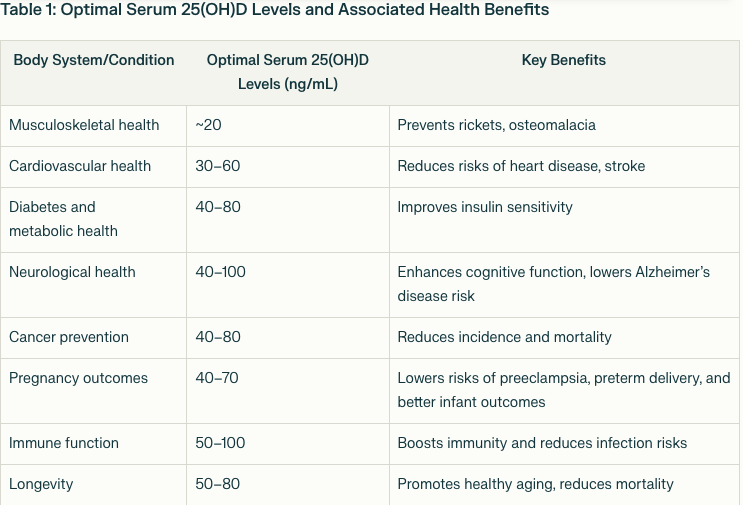
Different tissues exhibit varying thresholds for adequate vitamin D diffusion from circulation. For example, musculoskeletal tissues function optimally at serum 25(OH)D levels of approximately 20 ng/mL, whereas the cardiovascular and gastrointestinal systems require 30–40 ng/mL concentrations. For immune system optimization, cancer prevention, and longevity, serum 25(OH)D levels exceeding 50 ng/mL are necessary [2, 3]. Table 1 presents the optimal serum 25(OH)D concentration ranges for various body systems and associated disorders.
Broad Health Benefits of Vitamin D
Vitamin D is indispensable for musculoskeletal health and reduces the risk and severity of numerous other diseases. The latter include cardiovascular diseases, diabetes, cancer, respiratory illnesses, chronic kidney disease, immune dysfunction, autoimmune conditions, neurological disorders such as Alzheimer’s disease, and complications during pregnancy [6].
Vitamin D deficiency (VDD) is widespread globally, even in regions with abundant sunlight.
In the United States, approximately 40% of the population has deficient 25(OH)D levels (<20 ng/mL), while rates in Central Europe exceed 50% [7]. In tropical regions such as South Asia and the Middle East, VDD prevalence surpasses 60%, primarily due to sun-avoidance behaviors and darker skin tones, which reduce vitamin D synthesis. VDD is a major contributor to increased morbidity and premature mortality across a range of health conditions [7].
Evidence Supporting Optimal Vitamin D Levels
Extensive clinical trials and observational studies have demonstrated robust associations between serum 25(OH)D levels and health outcomes. Maintaining 40–80 ng/mL concentrations is critical for protecting against infections, autoimmune diseases, and chronic conditions [1, 8]. These levels far exceed the outdated 20–30 ng/mL recommendations from bodies like the NIH, IoM (USA), NICE, and SCAN (UK). Current guidelines focus on skeletal benefits while neglecting broader systemic advantages—they must be replaced.

Limitations of Current Guidelines and Large Trials
Many recent randomized controlled trials (RCTs) evaluating vitamin D have failed to demonstrate benefits due to inherently flawed designs. Common issues include inadequate participant selection resulting from the failure to measure baseline serum 25(OH)D levels [9], inconsistent supplementation dosages, and the inclusion of over-the-counter vitamin D use among study participants. Additional flaws include administering a single large dose without follow-up daily supplementation and using dosing intervals that are either too infrequent or too prolonged [10].
With most nutrients, RCTs are inappropriate for evaluating the efficacy and adverse effects of micro-nutrients. Unlike pharmacological agents, nutrients function as threshold substances—once a physiological plateau is reached, additional intake provides no further benefit. Consequently, researchers should prioritize well-designed, prospective, community-based clinical studies. Unfortunately, vitamin D guidelines have relied too heavily on flawed RCTs, leading to inadequate clinical recommendations. Notably, recent large trials and guidelines, including the Endocrine Society’s 2024 guidelines, have overlooked vitamin D’s extra-skeletal benefits and recommended insufficient supplementation doses of 600–800 IU/day.
Personalized Supplementation Strategies
The following straightforward calculations provided an easy way to accurately estimate an individual’s daily vitamin D requirement. Personalized supplementation based on body weight or BMI is recommended to achieve optimal serum 25(OH)D levels (Wimalawansa, SJ, Nutrients, 2022: https://doi.org/10.3390/nu14142997). A simplified formula categorizes dosage requirements:

Non-obese individuals (BMI < 29): 70–90 IU/kg/day
Moderately obese (BMI 30–39): 100–130 IU/kg/day
Morbidly obese (BMI ≥ 40): 140–180 IU/kg/day
Recommendations for Public Health
From a disease prevention perspective, non-obese adults (~70 kg) require a daily intake of 5,000–7,000 IU to maintain optimal serum 25(OH)D levels. Overweight and obese individuals need two to four times this amount due to volumetric dilution and sequestration in adipose tissue. Regular measurement of serum 25(OH)D is essential for at-risk populations, including older adults, pregnant women, individuals with darker skin tones, institutionalized persons, and those living in higher latitudes.
Broader implementation of food fortification programs (including deficient macro-nutrients) for nutrient-deficient, targeted populations is cost-effective in addressing widespread deficiencies. These programs, tailored to regional dietary habits, can significantly improve population-level vitamin D status and better health.
Conclusion
Vitamin D is an undervalued yet highly cost-effective natural agent with extensive health benefits beyond bone health. Despite mischaracterizations by conflicted scientists and physicians, evidence strongly supports its role in reducing the incidence and severity of various diseases and preventing premature deaths. There is an urgent need to revise the flawed vitamin D guidelines in most countries. Recommendations should focus on achieving serum 25(OH)D levels of 40–80 ng/mL through appropriate supplementation, routine screening, and safe sun exposure guidance. Implementing these measures can significantly reduce disease burdens, enhance longevity, lower healthcare costs, and improve global public health outcomes.
Funding: No funding was received for this work.
Conflicts of interest: None
https://www.researchgate.net/profile/Sunil-Wimalawansa/research
https://truthsocial.com/@SJWimalawansa
https://www.facebook.com/sunil.wimalawansa/
References:
Wimalawansa, S.J., Physiological Basis for Using Vitamin D to Improve Health. Biomedicines, 2023. 11(6).
Wimalawansa, S.J., Rapidly Increasing Serum 25(OH)D Boosts the Immune System, against Infections-Sepsis and COVID-19. Nutrients, 2022. 14(14).
Wimalawansa, S., Overcoming infections including COVID-19, by maintaining circulating 25(OH)D concentrations above 50 ng/mL. Pathology & Lab. Medicine Int., 2022. 14: p. 37–60.
Hollis, B.W., et al., Circulating vitamin D3 and 25-hydroxyvitamin D in humans: An important tool to define adequate nutritional vitamin D status. J Steroid Biochem Mol Biol, 2007. 103(3-5): p. 631-4.
Wimalawansa, S.J., Physiology of Vitamin D-Focusing on Disease Prevention. Nutrients, 2024. 16(11).
Wang, H., et al., Vitamin D and chronic diseases. Aging Dis, 2017. 8(3): p. 346-353.
Johnson, D.D., et al., Vitamin D deficiency and insufficiency is common during pregnancy. Am J Perinatol, 2011. 28(1): p. 7-12.
Wimalawansa, S.J., Infections and Autoimmunity-The Immune System and Vitamin D: A Systematic Review. Nutrients, 2023. 15(17).
Wimalawansa, S.J., S.T. Weiss, and B.W. Hollis, Integrating Endocrine, Genomic, and Extra-Skeletal Benefits of Vitamin D into National and Regional Clinical Guidelines. Nutrients, 2024. 16(22).
Grant, W., Wimalawansa SJ, Pludowski P, Cheng R, Vitamin D: Evidence-based health benefits and recommendations for population guidelines. Nutrients, 2025. 17(2): p. 277.
No mention of vitamin K2 to prevent D3 promoting calcification?
To read further research on vitamin D3 cholecalciferol supplementation and the need for 50 ng/mL (125 nmol/L = 1 part in 20,000,000 by mass) circulating 25-hydroxyvitamin D calcifediol, please see: https://vitamindstopscovid.info/00-evi/.
Attaining this level is so important that I suggest the IMA develop a vitamin D3 protocol, which is applicable to everyone, of all ages.
While infants who are substantially breast fed by 25-hydroxyvitamin D replete moms can obtain sufficient vitamin D3 and 25-hydroxyvitamin D for good health in breast milk, no other food sources contain more than a small fraction of the vitamin D3 required to maintain 50 ng/mL or more 25-hydroxyvitamin D in the bloodstream. (This 25-hydroxyvitamin D is made, over several days, primarily in the liver, by hydroxylating vitamin D3 at the 25th carbon. This is what is tested in "vitamin D" blood tests. Neither of these compounds are hormones - they are not signaling molecules.)
The centerpiece of such a protocol should be Prof. Wimalawansa's average daily vitamin D3 supplemental intake quantities, as specified above as three range of ratios of body weight. The first range, 70 to 90 IU vitamin D3 a day per kilogram body weight, suits everyone except those suffering from obesity. Higher ratios are needed for those suffering from obesity, since this reduces the rate of hydroxylation in the liver and the excess adipose tissue absorbs both vitamin D3 and 25-hydroxyvitamin D: https://vitamindstopscovid.info/00-evi/#obesity-deficit.
These recommendations should be followed by all people, unless there is medical advice to the contrary, with the exception of the breast babies just mentioned and those who have such high levels of ultraviolet-B skin exposure that they generate sufficient vitamin D3 in their skin to attain 50 ng/mL or more circulating 25-hydroxyvitamin D all year round. Far from the equator, such UV-B is not naturally obtainable except in the middle of cloud-free summer days, without glass, clothing or sunscreen intervening. Those with brown or especially black skin require very high levels of UV-B to generate sufficient vitamin D3 for full health.
Although general and skin exposure to sunlight has health benefits, and although in the absence of vitamin D3 supplementation, modest UV-B exposure is healthy, since it substantially raises otherwise terribly low 25-hydroxyvitamin D levels, all such UV-B exposure damages DNA and so raises the risk of skin cancer.
If we had no supplemental vitamin D3, health would be optimised by some level of UV-B skin exposure which trades off the skin cancer risk against the essential benefits of improving immune system function by raising 25-hydroxyvitamin D levels. However, since vitamin D3 is so inexpensive and readily available, the best approach is to supplement properly and avoid excessive UV-B exposure.
For average weight adults, 5000 to 7000 IUs (International Units) a day sounds like a lot - especially in countries like Australia where the greatest capacity capsule available over the counter is 1000 IU (25 micrograms). An IU is 1 40,000,000th of a gram. 5000 IU(125 micrograms = 1/8th of a milligram) a day is a gram every 22 years. Pharma-grade vitamin D3 costs about USD$2.50 a gram, ex-factory. (A credit card weighs about 5 grams.)
Proper vitamin D3 supplementation, without risk of toxicity and without the need for blood tests or medical monitoring, as Prof. Wimalawansa recommends, is by far the most important single step which most people can take to improving their health, since without this many people, at least in winter, have half or less of the 25-hydroxyvitamin D their immune system needs to function properly. Some - especially those with brown or black skin, the elderly and/or those with sun-avoidant lifestyles - have levels as low as 5 ng/mL (12.5 nmol/L).
Inadequate vitamin D3 supplementation during pregnancy, and so low 25-hydroxyvitamin D levels, raise the risk of pre-eclampsia, pre-term birth, autism, mental retardation: https://vitamindstopscovid.info/00-evi/#3.2, drives infectious and chronic inflammatory diseases and condemns many to cognitive decline -> dementia in old age https://vitamindstopscovid.info/00- evi/#3.3).
For those facing critical illness such as sepsis, severe COVID-19, Kawasaki disease, MIS-C (PIMS), ARDS etc. and who have today's very common, low 25-hydroxyvitamin D levels, there is an urgent need to boost this level in such clinical emergencies. Daily supplemental intakes of vitamin D3 in quantities Prof. Wimalawansa recommends take months to raise the level of circulating 25-hydroxyvitamin D to 50 ng/mL.
A crucial part of a future IMA vitamin D3 protocol would be boosting this level with a single oral dose of calcifediol - which *is* 25-hydroxyvitamin D. The amount required is not critical but Prof. Wimalawansa recommends 0.014 milligrams (14 micrograms) of calcifediol per kilogram body weight. For 70 kg 154 pounds, this is 1 milligram.
Calcifediol is more readily absorbed into the bloodstream than vitamin D3 since it has two hydrophilic hydroxyl group, while vitamin D3 has only one. It goes straight into circulation as the 25-hydroxyvitamin D many types of immune cell need to run their intracrine (inside each cell) and paracrine (to nearby cells, typically of different types) signaling systems. These systems are crucial to the ability of individual immune cells to respond to their changing circumstances.
A bolus (loading) dose of vitamin D3 is the next best approach is calcifediol is not available. (Packets of ten 0.266 mg calcifediol capsules are available over the counter in countries including Spain and Italy - but 0.01 mg is the highest amount available per tablet without prescription in the USA: https://dvelopimmunity.com/products/vitamin-d-times-three.)
For average weight adults, 10 mg (400,000 IU) vitamin D3 is a good amount. Only about 1/4 of this is hydroxylated in the liver to circulating 25-hydroxyvitamin D - and this takes several days. Critically ill patients are fighting for their lives, so every hour counts. 1 milligram of oral calcifediol will raise the 25-hydroxyvitamin D level of average weight adults, from any low level to at least 50 ng/mL in four hours or less.
This treatment alone would have saved the great majority of people who died from COVID-19, and of the 11 million or so people worldwide a year who are killed by sepsis: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)32989-7/fulltext.
In Cordoba, Spain (https://vitamindstopscovid.info/00-evi/#castillo https://www.sciencedirect.com/science/article/pii/S0960076020302764) an initial dose of 0.532 milligrams calcifediol for hospitalized COVID-19 patients was the primary reason, in the Castillo et al. RCT, for ICU admissions dropping from 50% to 2% and deaths from 8% to zero.
Ivermectin is the best known early treatment for COVID-19, but this calcifediol treatment is even more beneficial.